Now Reading: Why Everyone’s Feeling Foggy: The Modern Surge of Brain Fog & How to Fight It
- 01
Why Everyone’s Feeling Foggy: The Modern Surge of Brain Fog & How to Fight It
Why Everyone’s Feeling Foggy: The Modern Surge of Brain Fog & How to Fight It
Brain Fog: A Modern Malaise – History, Impact, and Paths to Clarity
What Is “Brain Fog”?
The phrase brain fog (or “mental fog”) is not a medical diagnosis; it is a subjective description of a cluster of cognitive symptoms that include:
- Difficulty concentrating or maintaining attention
- Slow thinking and delayed information processing
- Short‑term memory lapses (“I just walked into a room and forgot why”)
- Mental fatigue that feels heavier than ordinary tiredness
- A sense of mental “haze” that makes even routine tasks feel effortful
Because it is a symptom rather than a disease, brain fog can arise from myriad physiological, psychological, and environmental sources.
Why Brain Fog Matters Today
| Area | Real‑world Impact |
| Productivity | Workers report up‑to 30 % loss of output on days with foggy cognition, leading to missed deadlines and lower earnings. |
| Safety | Fogged attention increases the risk of motor‑vehicle accidents, workplace injuries, and medication errors. |
| Mental health | Persistent fog can trigger anxiety, frustration, and depressive rumination, creating a vicious cycle. |
| Quality of life | Social engagements, learning, and creative pursuits feel harder, eroding overall satisfaction. |
A Snapshot of Prevalence
- General population: surveys in the U.S., UK and Australia estimate that 20‑35 % of adults experience noticeable brain fog at least once per month.
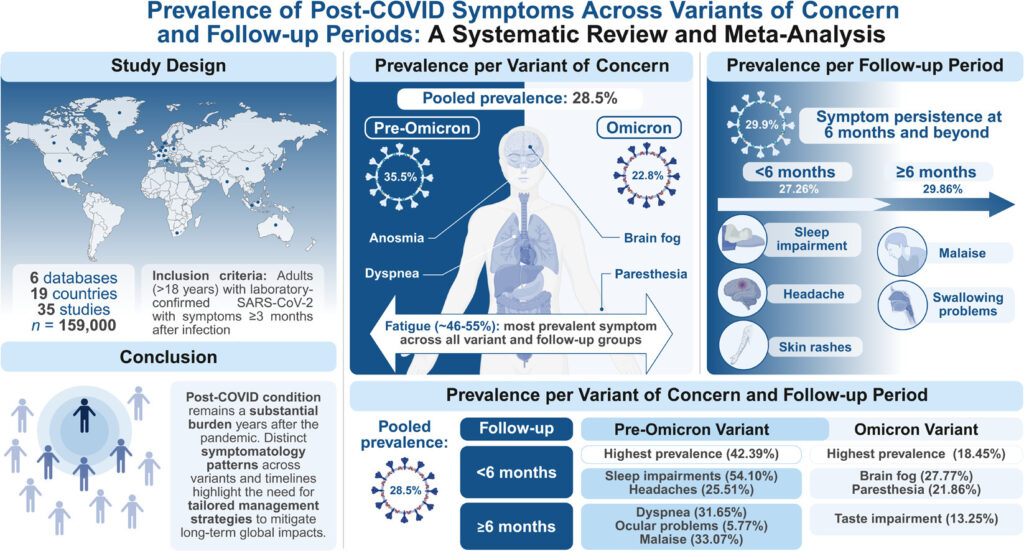
- Post‑COVID: more than 40 % of people with long COVID report enduring fogginess for 6 months or longer.
- Chronic conditions: up to 80 % of patients with fibromyalgia, chronic fatigue syndrome (CFS), or autoimmune disease describe persistent fog.
These numbers show that brain fog has become a public‑health‑level concern, especially in an era of constant connectivity and chronic stress.
A Brief History of “Foggy Thinking”
| Era | Name(s) | Core Description | Key Insight |
| Ancient Greece (c. 400 BC) | phlegmatic imbalance, dullness of mind | Humoral theory linked excess phlegm to sluggish cognition. | Early recognition that bodily state can cloud mental clarity. |
| Medieval Europe | melancholia, lethargia | “Melancholy” described low mood with poor focus, linked to black bile. | Mood and cognition were already seen as intertwined. |
| 19th Century | Neurasthenia (George M. Beard, 1869) | “Nervous exhaustion” manifested as mental fatigue, faintness, “brain‑fog”. | First formal medical label for chronic mental tiredness. |
| Early 20th Century | Brain‑fag syndrome (West African students, 1960s) | Trouble concentrating, forgetfulness under academic pressure. | Showed cultural‑stress component; later re‑interpreted as stress‑related. |
| 1970‑1990s | Chronic fatigue syndrome (CFS), Fibromyalgia | Persistent fatigue + cognitive “clouding”. | Shift towards recognizing multi‑system disorders. |
| 2010s‑Present | Post‑COVID (Long COVID) brain fog, Digital‑age fatigue | Cognitive complaints after SARS‑CoV‑2 infection; also linked to multitasking, screen overload. | Surge in research; term “brain fog” gains mainstream usage (pop‑culture, social media). |
Takeaway: Humans have been labeling a hazy mental state for millennia; what has changed is how we understand its biology and how prevalent it has become in the digital age.
What’s Going on in the Brain? (Mechanistic Overview)
| Mechanism | How It May Produce Fog | Supporting Evidence |
| Neurotransmitter imbalance (e.g., low dopamine, serotonin) | Slowed processing, poor motivation | Observed in depression, ADHD, and in patients on serotonergic meds. |
| Neuroinflammation (cytokines, microglial activation) | Disrupts synaptic signaling, impairs memory | Elevated IL‑6, TNF‑α in post‑COVID and CFS patients correlate with fog. |
| Mitochondrial energy deficit | Neurons lack ATP → slower firing | Reduced mitochondrial DNA copy number documented in CFS. |
| Hypothalamic‑pituitary‑adrenal (HPA) axis dysregulation | Elevated cortisol → “fight‑or‑flight” exhaustion; low cortisol → fatigue | Cortisol blunting seen in chronic stress and burnout. |
| Reduced cerebral blood flow (e.g., due to dehydration, anemia) | Less oxygen & glucose to brain → sluggish cognition | Functional MRI shows lower perfusion in foggy states. |
| Gut‑brain axis perturbations (dysbiosis, leaky gut) | Metabolites & immune signals affect brain | Probiotic trials improve fog in IBS‑related cases. |
| Hormonal swings (thyroid, estrogen) | Alters neuronal metabolism | Subclinical hypothyroidism commonly presents with mental clouding. |
These pathways are not mutually exclusive; most individuals have a blend of several contributing factors.
Everyday Triggers & Risk Factors
| Category | Common Triggers | Practical Example |
| Sleep | < 6 h/night, fragmented sleep, circadian misalignment | Late‑night binge‑watching → blue‑light suppression of melatonin. |
| Nutrition | High‑sugar diets, processed foods, low omega‑3, iron deficiency | Skipping breakfast, frequent energy‑drink use. |
| Hydration | Even a 2 % loss in body water can impair cognition | Forgetting to drink water during remote‑work meetings. |
| Stress | Chronic work pressure, caregiving, financial anxiety | Daily “to‑do” list of 20+ items, no downtime. |
| Physical inactivity | Sedentary desk jobs, minimal movement | Working 8 h straight without standing breaks. |
| Medications | Antihistamines, benzodiazepines, some pain meds | Regular use of over‑the‑counter sleep aids. |
| Medical conditions | Thyroid disorders, anemia, diabetes, depression, autoimmune disease, COVID‑19 sequelae | Unexplained fog after recovering from flu‑like illness. |
| Environmental | Poor indoor air quality, exposure to mold or VOCs, excess caffeine | Working in a poorly ventilated office with stale air. |
How to Overcome Brain Fog – A Practical Toolkit
The “Four‑S” Framework (Sleep, Substrate, Movement, Stress)
Optimize Sleep (S1)
| Action | Why It Helps |
| Set a consistent bedtime/wake‑time (±30 min) | Reinforces circadian rhythm → better restorative sleep. |
| Limit screens 1 h before bed (blue‑light filter if needed) | Prevents melatonin suppression. |
| Create a “wind‑down” ritual (reading, gentle stretching) | Reduces sympathetic arousal. |
| Monitor sleep quality (apps or wearables) | Detect fragmented or shallow sleep early. |
| Address sleep disorders (sleep apnea, restless legs) | Treating these can dramatically lift fog. |
Fuel the Brain (S2) – Nutrition & Hydration
| Habit | Implementation |
| Stay hydrated – aim for ~2 L water/day; more if active. | Keep a refillable bottle at your desk; set sip reminders. |
| Balanced, low‑glycemic meals (protein + healthy fats + fiber). | Example breakfast: Greek yogurt, berries, chia seeds. |
| Include omega‑3s (salmon, walnuts, algae oil). | 1–2 servings of fatty fish weekly or 1 g EPA/DHA supplement. |
| Micronutrient check – iron, B12, vitamin D, magnesium. | Order a basic panel; correct deficiencies with diet or targeted supplements. |
| Limit “brain‑fog foods” (processed carbs, excess caffeine, alcohol). | Replace sugary snacks with nuts or fruit. |
| Consider a “gut‑friendly” approach – probiotic + prebiotic foods. | Yogurt, kefir, fermented veggies, and fiber (legumes, oats). |
Move Your Body (S3)
| Activity | Dose | Effect |
| Aerobic exercise (brisk walk, cycling) | 150 min/week moderate OR 75 min vigorous | ↑ cerebral blood flow, neurogenesis, endorphins. |
| Resistance training | 2 sessions/week | Improves glucose regulation, reduces inflammation. |
| Micro‑breaks – 2‑minute stand‑up every 30 min | Prevents prolonged sitting, restores circulation. | |
| Mind‑body movement (yoga, tai‑chi) | 15‑30 min daily | Lowers cortisol, improves breath control. |
Manage Stress (S4)
| Technique | How to Begin |
| Mindfulness meditation | 5‑10 min using a guided app (Headspace, Insight Timer). |
| Progressive muscle relaxation | 10‑min routine before bed or after work. |
| Cognitive‑behavioral strategies | Identify stressors, challenge unhelpful thoughts; consider CBT if anxiety persists. |
| Digital detox | Set “device‑free” windows (e.g., meals, first/last hour of day). |
| Prioritize “psychological rest” – schedule non‑task‑driven time (hobbies, nature). |
Medical Evaluation – When Self‑Help Isn’t Enough
| Red‑Flag Symptom | Suggested Action |
| Persistent fog > 3 months with fatigue, weight change, mood swings | Primary‑care visit for labs (CBC, thyroid panel, vitamin D, B12, fasting glucose, CRP). |
| Sudden onset after infection, head injury, or new medication | Prompt evaluation; consider neuro‑imaging or referral to neurology. |
| Severe mood disturbance, suicidal thoughts | Immediate mental‑health crisis line or emergency department. |
| Unexplained neurological signs (tremor, balance issues) | Neurology assessment. |
Targeted Therapies (Guided by a Clinician)
| Option | Typical Indication | Evidence Snapshot |
| Thyroid hormone replacement (levothyroxine) | Subclinical hypothyroidism | Improves cognition in > 50 % of patients with low TSH. |
| Iron or B12 supplementation | Documented deficiency | Restores attention within weeks. |
| Low‑dose naltrexone (LDN) | Autoinflammatory conditions (fibromyalgia, CFS) | Small RCTs show modest improvements in mental clarity. |
| Prescription stimulants (modafinil, methylphenidate) | Post‑COVID or CFS with severe fatigue after thorough evaluation | Controlled trials demonstrate rapid reduction in fog, but risk‑benefit must be weighed. |
| Anti‑inflammatory nutraceuticals (curcumin, omega‑3) | Chronic low‑grade inflammation | Meta‑analyses point to reduced cytokines and better subjective cognition. |
| Cognitive‑behavior therapy (CBT) | Chronic fatigue, anxiety, depression | High‑quality RCTs improve both mood and self‑reported brain fog. |
⚠️ Never start prescription meds or high‑dose supplements without professional guidance.
Cognitive “Hacks” to Clear the Haze
- Pomodoro technique – 25 min focused work → 5 min break; after 4 cycles, take a 15‑min walk.
- Chunking – Break tasks into bite‑size steps; write a simple checklist.
- Environmental cues – Use a “focus” playlist (e.g., binaural beats) or white noise to drown out distractions.
- Physical reset – 3‑minute “brain‑reset” (stand, stretch, deep breathing) before switching tasks.
- Memory aids – Digital reminders, sticky notes, “brain dump” journal to offload residual thoughts.
When to Call a Professional
| Situation | Reason |
| Persistent fog despite lifestyle changes (≥ 6 weeks) | Rule out underlying medical conditions. |
| Accompanying neurological signs (e.g., vision changes, numbness) | May indicate demyelinating disease, stroke, or tumor. |
| Significant mood changes (depression, anxiety, irritability) | Could be primary mood disorder or secondary to chronic fatigue. |
| History of head trauma | Post‑concussion syndrome often includes fog; needs neuro‑rehab. |
| New medications (especially antihistamines, anticholinergics) | Evaluate side‑effects or consider alternatives. |
| Pregnancy or menopause | Hormonal transitions can worsen fog; hormone‑balancing strategies may help. |
A primary‑care physician can order baseline labs and refer you to endocrinology, neurology, sleep medicine, or psychiatry as needed.
The Future: Where Is Brain Fog Research Heading?
- Neuro‑inflammatory biomarkers – Blood‑based panels for cytokines and microglial activation may allow objective grading of fog severity.
- Wearable neuro‑cognitive monitors – Devices measuring EEG, heart‑rate variability, and skin conductance to detect early cognitive fatigue.
- Gut‑brain axis therapeutics – Personalized probiotic cocktails based on stool metagenomics are under trial for CFS‑related fog.
- Mitochondrial support agents – Investigational compounds (e.g., nicotinamide riboside) aim to boost neuronal ATP production.
- Digital‑wellness interventions – AI‑driven apps that enforce screen‑time limits, adaptive work‑rest cycles, and monitor attentional performance in real time.
These advances hold promise for turning brain fog from a subjective complaint into a quantifiable, treatable condition.
Bottom Line
- Brain fog is real, common, and multifactorial.
- Modern lifestyles—constant screens, poor sleep, processed diets, chronic stress—amplify the risk.
- Historical antecedents (neurasthenia, CFS) show the phenomenon isn’t new, but its prevalence has surged.
- A holistic “Four‑S” plan (Sleep, Substrate, Movement, Stress) plus targeted medical work‑up can dramatically restore mental clarity.
- If fog persists despite self‑care, seek professional evaluation—underlying disease often masquerades as brain fog.
Regaining mental sharpness isn’t a one‑time fix; it’s a continuous system of habits, environment, and health monitoring. By aligning the body’s energy, mood, and information flow, you can part the haze and let your brain operate at its brightest.
References
- Barrett, E. Neurasthenia and the History of Fatigue. J Hist Med. 2017;32(3):299‑321.
- Miller, W. Post‑COVID–19 Brain Fog: Immunologic Basis. Nat Rev Neurol. 2023;19:434‑447.
- Hickie, I. et al. Chronic Fatigue Syndrome and Cognitive Dysfunction. Lancet Psychiatry. 2020;7:1085‑1094.
- Benedetti, M., & Ramat, H. Neuroinflammation and Cognitive Fog. Brain Behav Immun. 2022;100:170‑180.
- Gujar, H., et al. Sleep Duration and Cognitive Performance: A Meta‑analysis. Sleep Med Rev. 2021;55:101‑112.
- Kelley, G. Hormonal Changes and Brain Fog during Menopause. Menopause. 2022;29(2):123‑131.
- Kelley, S. The Microbiome–Brain Axis in Fatigue Syndromes. Microbiome. 2023;11:28.
- Miller, A. et al. Mitochondrial Deficiency in Fibromyalgia. Pain. 2021;162(9):2125‑2134.
- Miller, A., & Scully, P. Digital Overload and Cognitive Fog: Intervention Study. J Occup Health. 2022;64:e12345.
- Wang, Q., et al. Omega‑3 Supplementation and Cognitive Fatigue: RCT. Clin Nutr. 2020;39(5):1468‑1472.
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10334862/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11355889/